Registered Health Care Practitioners are responsible for:
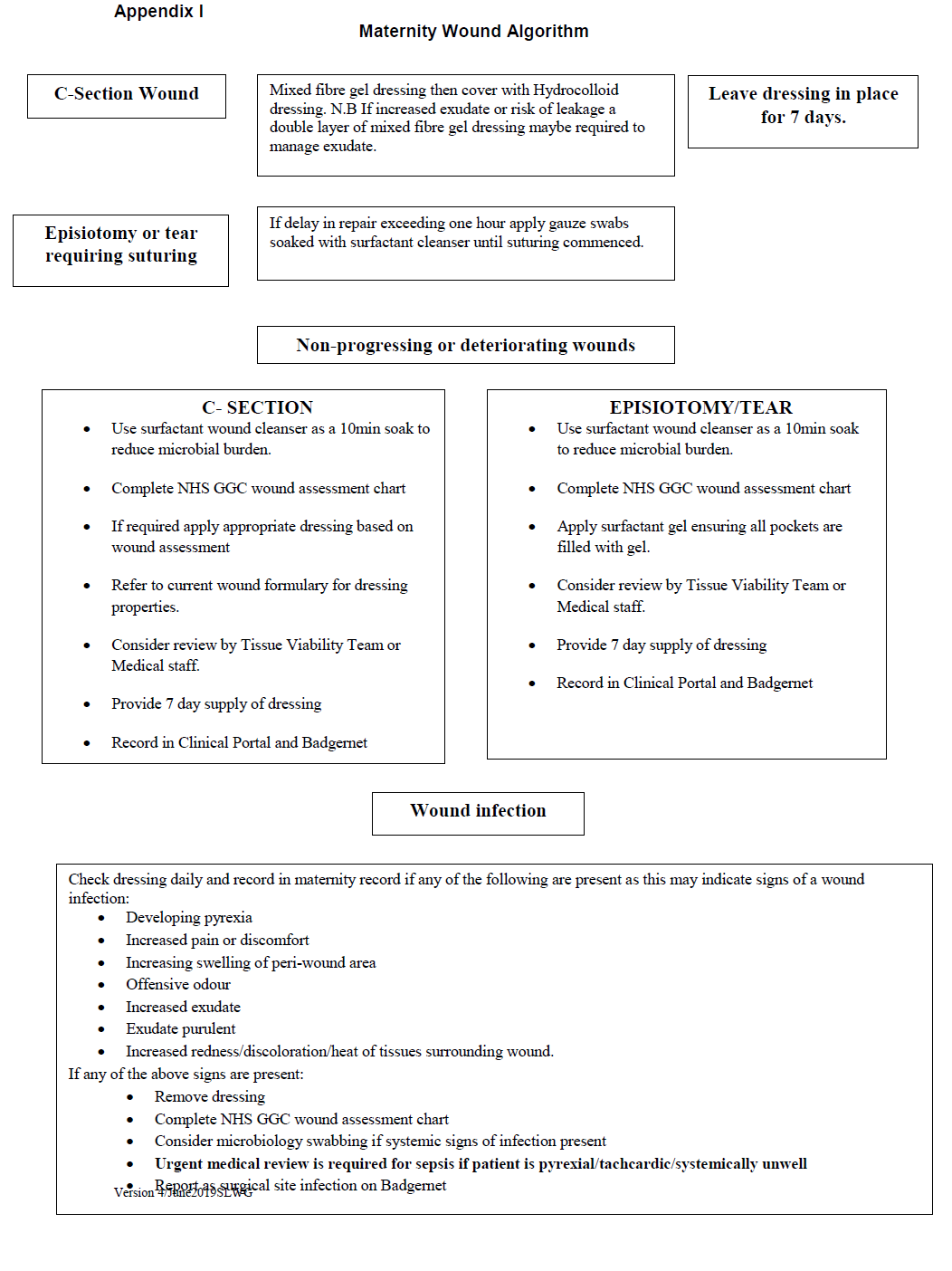
- Informing women of the wound dressing protocol in the event of a caesarean section and informing of appropriate wound care post caesarean section/episiotomy/tear suturing.
- Liaising with carers and the interdisciplinary team to promote compliance of dressing protocol, ensuring that Interdisciplinary Women Focused Care Plans are in place and interventions are recorded and dated in line with the Board’s Record Keeping Policy.
- Maintaining and updating their knowledge, skills and competence in line with their roles and responsibilities to care for women who undergo caesarean section, episiotomy or tear suturing.
- Seeking the advice of the Tissue Viability Service where appropriate, whilst maintaining ongoing responsibility for the woman’s episode of care.
- Referring all non-progressing wounds after two weeks to the Tissue Viability Service.